K. Manal1, B. Misialek1, B. Li2, P. Jenks3, B. Gillette3, I. Lockwood3
1KTM LLC, Newark, DE. 2enCore Laboratory, Santa Ana, CA. 3Accudyne Systems Inc, Newark, DE.
INTRODUCTION
The keyboard and mouse are the most widely used computer input devices. Individuals with severe upper limb paralysis (SULP) with little to no manual dexterity require alternate modes of computer input to benefit from technologies used by non-disabled persons. Alternate input devices, broadly grouped as assistive technologies (AT), allow people with SULP to substitute manual dexterity with other intact motor capabilities to direct cursor movements and initiate mouse-clicks. There is a broad range of AT used by people with SULP, and these technologies differ markedly in terms of complexity, function, and effectiveness. Eye tracking for example is a technically sophisticated and effective mode of input, however the cost can be prohibitive to many. Sip-and-puff switches are at the opposite end of the cost-effectiveness continuum but are nonetheless a valued and reliable mode of input used by many people with SULP.
Computer access using tongue control is an underutilized physical option for individuals with SULP. To the best of our knowledge there are no tongue-controlled computer input devices on the market. The tongue drive system (TDS) developed at Georgia Tech showed promising results demonstrating feasibility of tongue control in a laboratory setting. The TDS tracks the position of a metallic tongue-piercing within the mouth using an array of magneto-resistive sensors. Moving the tongue-piercing to predefined locations within the mouth directs cursor movement in one of four cardinal directions (up, down, left & right), with a dwell timer used for object selection. Throughput (TP), a measure of the information delivered to the computer through the input device, was greater for individuals with tetraplegia performing a center-out-tapping test using the TDS compared to the sip-and-puff controller they were accustomed to using. [1]
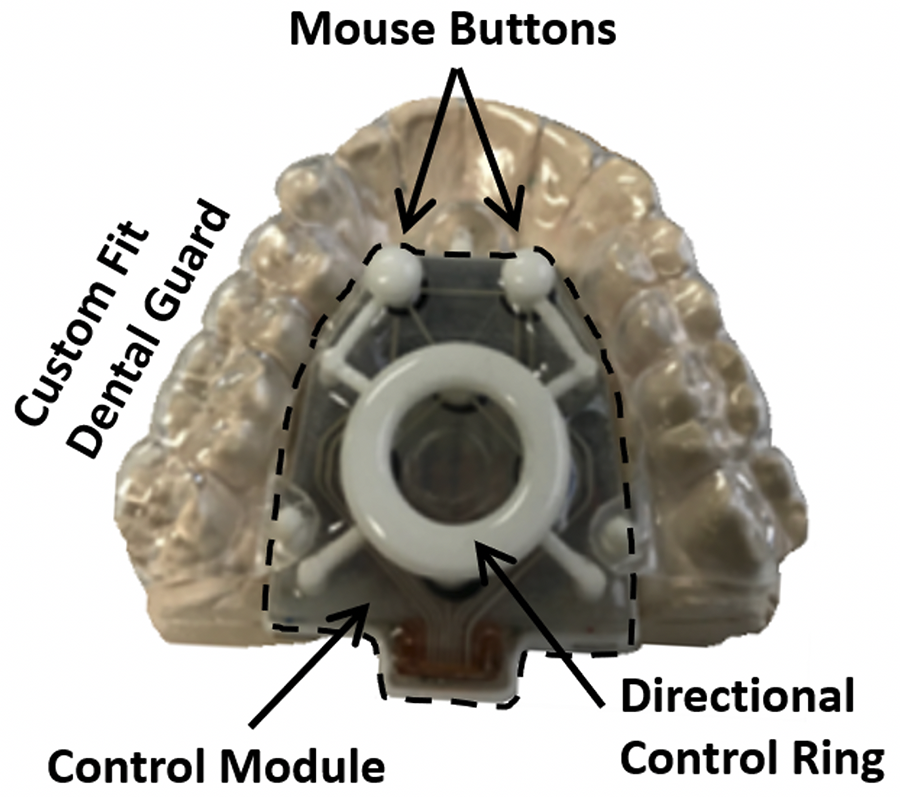
The Mouth Mouse is an alternate tongue-controlled computer input device being developed with SBIR Phase II funding from NIDILRR. The Mouth Mouse uses forces sensitive resistors (FSRs) to direct cursor movement and initiate left and right mouse clicks. It is a proportional controller capable of straight line, diagonal and curved cursor trajectories based on the position and magnitude of tongue force applied to a directional control ring resting on the directional FSR's (Figure 1).
In this paper we report performance data for able-bodied participants performing a multidirectional tapping task using the Mouth Mouse and a standard computer mouse. Throughput was evaluated over 5 testing sessions to monitor learning effects that were expected when using a novel device. Participants filled-out the System Usability Survey (SUS) after testing session 5 subjectively evaluating usability of the Mouth Mouse as a computer input device. [2] In addition, TP for the Mouth Mouse was compared to published values for the TDS evaluated under similar test conditions. We hypothesized the Mouth Mouse would be a more effective controller because it is not limited to straight line sequential paths as the TDS.
METHODS
| D/A | 128 | 256 | 512 |
| 26 | 2.57 | 3,44 | 4.37 |
| 52 | 1.79 | 2.57 | 3.44 |
| 104 | 1.16 | 1.79 | 2.57 |
Ten (7F / 3M) able-bodied participants (mean 27.2 ± 8.2 yrs) were asked to complete five test sessions within a two-to-three-week period. Each test session involved three trials of multidirectional tapping as outlined in ISO-9241, Part 9. [3] Each participant performed the multidirectional tapping test using the Mouth Mouse and a standard computer mouse. The study was approved by the Biomedical Research Alliance of New York. All participants provided informed consent prior to enrollment in the study.
Mouth Mouse Multidirectional Tapping
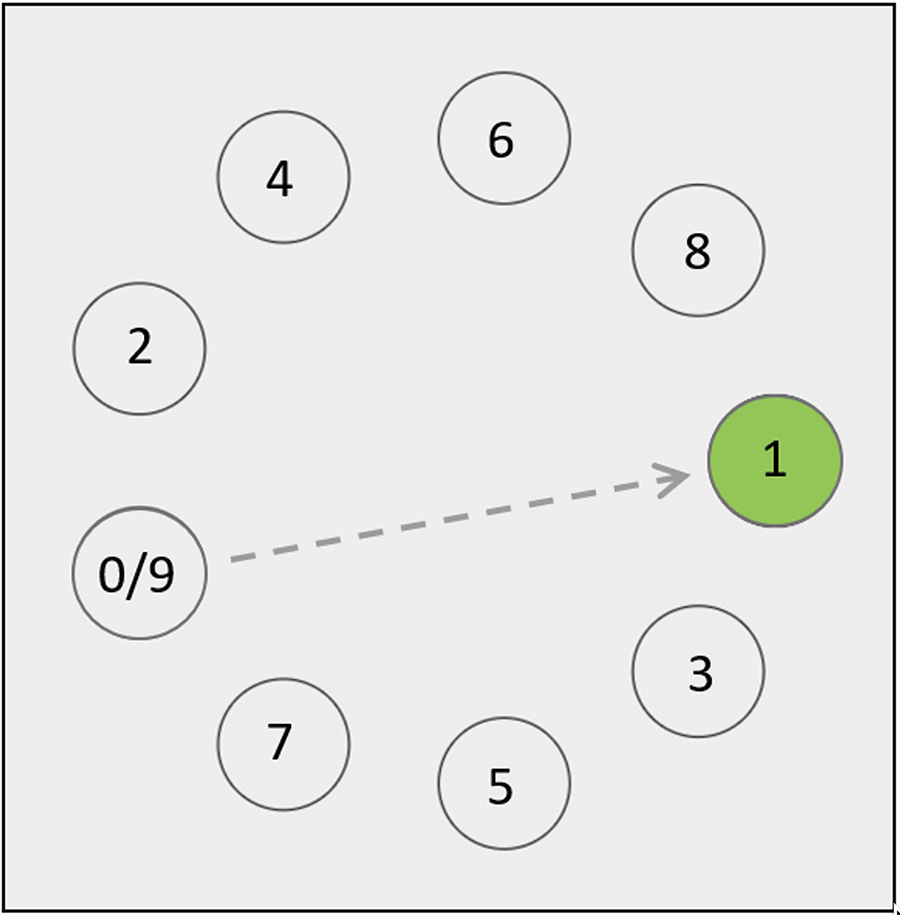
Each trial consisted of 9 sequences of 9 targets spaced evenly around the perimeter of a circle. The 9 sequences included three different target diameters (D), and three different amplitudes (A) between targets. Target diameters and amplitudes are listed in Table 1, with the corresponding index of difficulty for each pairing. The goal of the multidirectional tapping task was to move the cursor as quickly and accurately to the center of each target and select it with a left mouse click. The cursor for each sequence always started from the 0-target position with the next move-to target highlighted in green. This pattern proceeded around the perimeter of the circle terminating with the last path from target 8 to target 9 (Figure 2). Each trial of 9 sequences consisted of 81 targets.
TDS Multidirectional Tapping
Nine able-bodied participants performed a 15-target multidirectional task using the TDS and a standard computer mouse. Two different target diameters (57 & 76 pixels) and amplitudes (305 & 534 pixels) were evaluated. The index of difficulty for these pairings ranged between 2.67 and 3.37.
The effective index of difficulty (IDe) for each pairing of D and A for the Mouth Mouse and the TDS is defined by equation 1,
(1)
where Ae is the mean movement amplitude along the task axis between targets and We is a measure of the spatial variability from the click point to the center of each target within a sequence. [3]
Throughput (TP), a measure of performance with units of bits/s, is calculated as the ratio of IDe and the mean movement time (MT) between targets within a sequence,
(2)
TP for the Mouth Mouse was averaged across the 9 sequences for each of the 3 trials and 10 subjects by test session. TP for the TDS was reported based on previously published values. [4]
| The System Usability Scale | |
| When a SUS is used, participants are asked to score the following 10 items with one of five responses that range from Strongly Agree to Strongly disagree: | |
| 1. | I think that | would like to use this system frequently. |
| 2. | I found the system unnecessarily complex. |
| 3. | I thought the system was easy to use. |
| 4. | I think that I would need the support of a technical person to be able to use this system. |
| 5. | I found the various functions in this system were well integrated. |
| 6. | I thought there was too much inconsistency in this system. |
| 7. | I would imagine that most people would learn to use this system very quickly. |
| 8. | I found the system very cumbersome to use. |
| 9. | I felt very confident using the system. |
| 10. | I needed to learn a lot of things before I could get going with this system. |
The system usability survey questions are listed in Figure 3. All 10 participants in our study completed the survey after session 5. No similar survey data was reported by GT for the TDS.
RESULTS
Figure 4 shows the average TP across subjects by session using the Mouth Mouse. TP increased by 118% between sessions 1 and 5. The most notable and consistent pattern of improvement was between sessions 1 and 2, with continued, albeit less improvement from session 2 through session 5. As a point of comparison TP using the computer Mouse averaged 4.74 ± 0.60 bits/s across test sessions.
TP for GT participants using a standard computer mouse was 4.52 ± 0.44 bit/s. There was no significant difference in TP for the computer mouse between studies [ t(17) = 0.902, p = 0.38]. This is not surprising given the similarity of the testing protocol with similar indices of difficulty. This finding was expected and supports the construct validity of comparing TP for the Mouth Mouse and TDS, even though data for these two devices were collected in different studies.
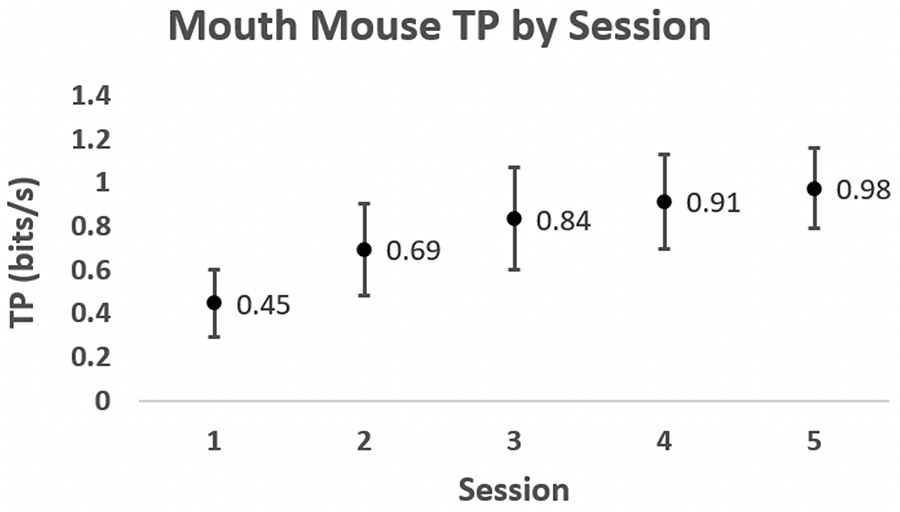
The mean TP for the Mouth Mouse and the TDS in session 5 was identical (1.0 ± 0.2 bits/s). Similarly, TP in sessions 1 for the Mouth Mouse and TDS were 0.4 ± 0.2 and 0.4 ± 0.1 respectively. A very similar rate of improvement across test sessions was observed for both the Mouth Mouse and TDS.
The increase in TP using the Mouth Mouse between sessions 1 and 5 can partially be attributed to minor improvements in IDe up through session 4, but was primarily driven by reduced MT between sessions (Figure 5). The modest improvement in IDe between sessions 1 through 4 was the result of slightly less spatial variability (i.e., better accuracy) moving the cursor to the center of the target.
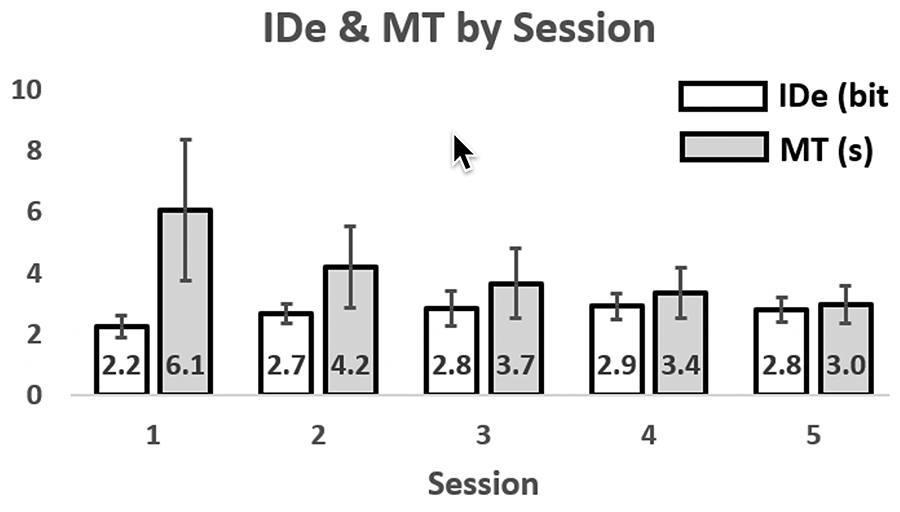
The mean MT between targets in session 1 was approximately 6 seconds. That is, the average time to complete a sequence of 9 targets in session 1 was approximately 55 seconds (9 targets x 6.1 s/target). In session 5 the mean MT between targets dropped to 3 seconds corresponding to an improvement of 100%. Not only did average MT decrease, variability in MT also decreased between sessions.
The overall SUS rating for the Mouth Mouse was 75.5 ±13.0 with a range of 60.0 to 97.5. A mean SUS score of 75.5 corresponds to an adjective classification of usability between good and excellent. [5] There was no relationship whatsoever between subject performance (i.e., TP) and an individual's SUS rating.
DISCUSSION
The Mouth Mouse is an alternate computer input device designed for individuals with SULP. The first step in evaluating whether the Mouth Mouse is a viable controller was to evaluate performance by participants for whom cognitive impairment would not be a confounding factor when learning to use the device. Preliminary data for 10 able-bodied participants with no known cognitive deficits suggests there is some degree of learning when first using the Mouth Mouse; most notably between sessions 1 and 2. Whether TP would have continued to improve with more exposure beyond session 5 is unknown, however it appears TP plateaued with a small reduction in variability between sessions 4 and 5. This information may be useful for individuals with SULP providing a realistic performance expectation when first learning to use the device.
It is noteworthy that a very similar learning curve to ours (i.e., TP by session) was reported for the able-bodied GT participants using the TDS. [4]. It is premature to conclude these similarities speak to the capacity of the lingual motor system to adapt to precisely positioning the tip of the tongue within the intraoral space. It does however suggest that able-bodied participants can learn to use fine tongue control as a mode for computer access.
Our hypothesis the Mouth Mouse would be a more effective controller than the TDS was not validated. There are several reasons this may be the case, and it is difficult to know for sure since data were collected in different studies. The Mouth Mouse is a true proportional controller with movement speed proportional to applied tongue force. In contrast, the TDS moves in sequential straight-line paths with a predefined cursor acceleration that immediately stops when the metal tongue piercing is positioned in the neutral position within the mouth, and it uses a dwell timer with a short selection interval (0.46 s) to automatically select the target. A video of a test subject performing the center-out-tapping tasks using the TDS shows the cursor rapidly approaching the target, stopping immediately and the target selected quickly with a brief dwell. In contrast, our participants tended to initially move rapidly toward the move-to target, slow down, and fine tune their approach before selecting the target with a left mouse click. Movement time in the calculation of TP for the TDS did not include the dwell time interval of 0.46 seconds, nor did it include any initiation delay before the subject moved the cursor. It was not possible to derive MT from the data reported by GT, but needless to say had they included the dwell time and initiation delay the overall TP for the TDS would have decreased, and possibly significantly.
Our subjects demonstrated the ability to generate diagonal and curved trajectories at a movement speed they controlled simply by varying the magnitude of tongue force applied to the control ring. This provides a high-degree of maneuverability and precision when moving the cursor. Physical mouse buttons eliminate the unintended dwell-timed selection of an object, giving the user the experience of selecting the object when they choose. It is worth noting the diameter of the smallest target in our study was approximately half the size of the smallest TDS target. The ability to precisely direct the cursor to a small target and select it with a user-selected mouse click may be especially relevant when trying to select a small target among many targets that are close together (e.g., an item on a small drop-down menu).
The next step in our evaluation of the Mouth Mouse will be to document performance and usability of the device by individuals with SULP. Previous work at GT showed that individuals with SULP did not perform as well as able-bodied subjects during a center-out-tapping task using the TDS. [1] This may be due to the targets appearing randomly, which makes motor-planning more challenging. Whether randomly appearing targets is the most informative way to evaluate performance of an input device is questionable, especially considering the static nature of the computing environment at a given time. That is, buttons, drop-downs, and links are in a fixed space at any one time and the user generally has full knowledge of where they intend to move before they need to do so. Nonetheless, the GT data suggest there may be a cognitive difference that affects performance between able-bodied participants and individuals with SULP assuming both groups had similar tongue control. This will be important to monitor in our future testing of the Mouth Mouse in an intended use group of participants with SULP.
CONCLUSION
Tongue control is an underutilized physical option for computer access by people with SULP. Our preliminary data suggest the Mouth Mouse is a viable option for people with intact tongue control and no cognitive impairment. Overall users accustomed to using a computer mouse rated usability of the Mouth Mouse between good and excellent. The results of this study support evaluation of the device in an intended use setting by individuals with SULP.
REFERENCES
[1] Kim J, Park H, Bruce J, Sutton E, Rowles D, Pucci D, Holbrook J, Minocha J, Nardone B, West D, Laumann A, Roth E, Jones M, Veledar E, Ghovanloo M. The tongue enables computer and wheelchair control for people with spinal cord injury. Sci Transl Med. 2013 27;5(213):213ra166.
[2] Brooke, J. SUS: A quick and dirty usability scale. In: Patrick W, Jordan PW, Thomas B, Weerdmeester BA, McClelland IL, editors. Usability Evaluation in Industry. 1996: pp. 189-194.
[3] Douglas SA, Kirkpatrick AE, Mackenzie SI. Testing Pointing Device Performance and User Assessment with ISO 9241, Part 9 Standard. Proceedings of the SIGCHI conference on Human Factors in Computing Systems. 1999.
[4] Yousefi B, Huo X, Veledar E, Ghovanloo M. Quantitative and comparative assessment of learning in a tongue-operated computer input device. IEEE Trans Inf Technol Biomed. 2011 15(5):747-757.
[5] Bangor A, Kortum P, Miller J. Determining What Individual SUS Scores Mean: Adding an Adjective Rating Scale. J.usability stud. 2009 4(3):114-123.