Stakeholder Satisfaction with Complex Rehabilitation Technology Maintenance and Repairs
Stephanie Chan1,2, Julia Parachini1,2, Tyler Beauregard1,2, Carmen P. DiGiovine, PhD ATP/SMS RET2,3,4,5
1 Ohio State University, School of Health and Rehabilitation Sciences
2 Ohio State University, Rehabilitation Engineering and Design Lab
3 Ohio State University, School of Health and Rehabilitation Sciences, Occupational Therapy Division
4 Ohio State University, College of Arts and Sciences, Speech and Hearing Sciences Department
5 Ohio State University Wexner Medical Center, Assistive Technology Center
INTRODUCTION
Complex rehabilitation technology (CRT) is an important group of wheelchair devices that assist individuals with disabilities to engage fully in their personal and professional lives. They are highly customizable and are crucial to assisting individuals with mobility impairing conditions to improve their quality of life.[1] CRT can include adaptive seating systems, customizable manual and power wheelchairs, and other mobility devices that are configured to meet the individual needs of the user.[2] The CRT service delivery process is complicated with multiple stakeholders and steps involved, and research has shown that there are barriers that prevent people with disabilities to obtain the device that they need efficiently and successfully. Currently, coverage of CRT by medical insurers are diagnosis driven and not based on the functional needs of the user, and the policies are also unnecessarily restrictive, only considering the medical needs of users in the home rather than their participation in the community as well, amongst other issues.[3] Previously, a scoping review completed by Betz et.al (2022) identified barriers and challenges that exist in the current CRT service delivery process.[2] Some of the barriers found included limited consumer training on use and maintenance of the device and lack of repair service. This was further discussed in Schmeler & Dicianno's (2022) article examining the scoping review, and it is mentioned that current CRT payment is based on a "fee for service" model where the supplier is paid in full for the device upon delivery, which means there is no obligation for the supplier to follow up and provide repair and maintenance services for the consumer. Furthermore, Centers for Medicaid and Medicare Services (CMS) does not provide coverage for device maintenance, and users are expected to maintain their own devices. This results in suppliers who provide repair services being inadequately reimbursed, and consumers also lacking the knowledge or physical capabilities to maintain their own devices.[3] The purpose of this paper is to describe the satisfaction with repair and maintenance of CRT devices across stakeholder groups involved in the CRT service delivery process.
METHODS
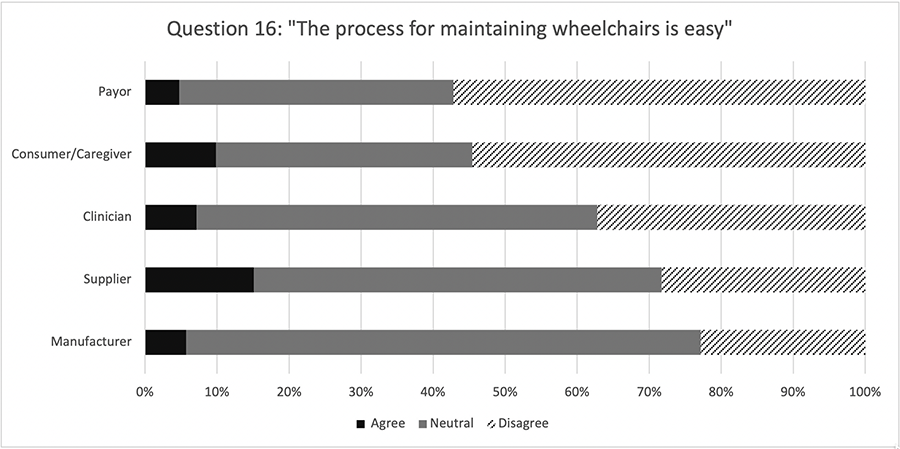
To investigate stakeholder's perception of various parts of the CRT service delivery process, a cross sectional, online questionnaire was developed.[4] The questions were developed around findings from the scoping review and steps of the Wheelchair Provision Guide developed by the Rehabilitation Engineering Society of North America (RESNA). This includes 1) Referral, 2) Assessment, 3) Equipment Recommendation and Selection, 4) Funding and Procurement, 5) Product Preparation, 6) Fitting, Training and Delivery, 7) Follow-up, Maintenance and Repair, and 8) Outcome Measurement.[5] There were 19 questions total, and respondents were able to answer each question on a 6-point Likert scale. Respondents also had the option to select the stakeholder group that they most closely identify with, as well as the geographic location that they reside in. The questionnaire was distributed to 42 organizations that were contacted by the project team, with representation from each stakeholder group.[4] For the purpose of examining repair and maintenance specifically, the questions that were based around Follow-up, Maintenance, and Repair (16,17, and 18) were analyzed by stakeholder group individually as well as aggregated to see stakeholder's perception towards each question and the theme of repair and maintenance as a whole. Instead of examining the responses by Likert scale, the responses were combined to either agree (positive), neutral, or disagree (negative). This was done by combining completely and mostly agree/disagree responses into agree or disagree, and somewhat agree and disagree into neutral. Question 18's (Figure 3) responses were flipped where a "disagree" response was considered positive and an "agree" response was negative, since the question was worded in a way where it was favorable for respondents to answer "disagree" to that question.
RESULTS
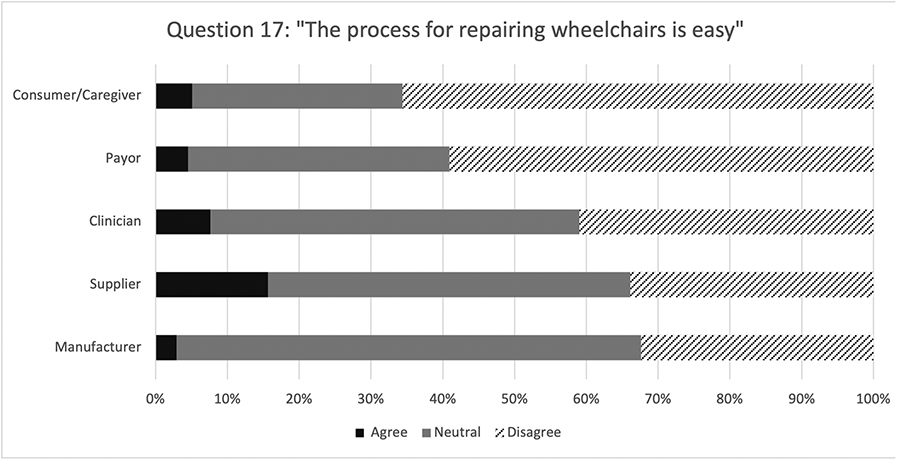
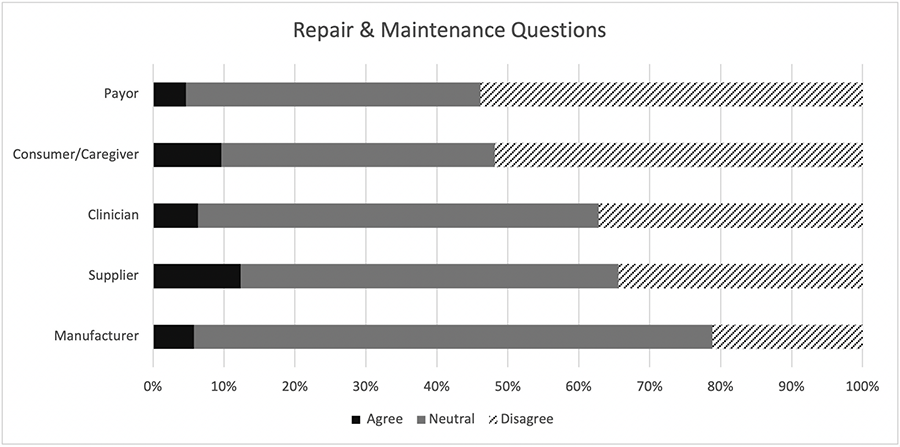
The questionnaire received a total number of 1069 responses, which consisted of 435 (40.7%) clinicians, 319 (29.8%) suppliers, 254 (23.8%) consumer/caregivers, 35 (3.3%) manufacturers, and 23 (2.2%) payors. There were 3 (0.3%) individuals who did not indicate a stakeholder group. Quantitative analysis of the individual questions that pertained to repair and maintenance (Figures 1-3) and the questions combined showed that all stakeholder groups (Figure 4) hold an overall negative attitude towards repair and maintenance of CRT devices in the service delivery process. Specifically, payors had the highest number of negative responses in 2 out of the 3 questions studied (over 50%), and manufacturers had the lowest number of negative responses in all 3 questions (less than 35%). There was not one stakeholder group who was positive about any of the questions studied, with none of the "agree" responses above 15% for any stakeholder group.
DISCUSSION
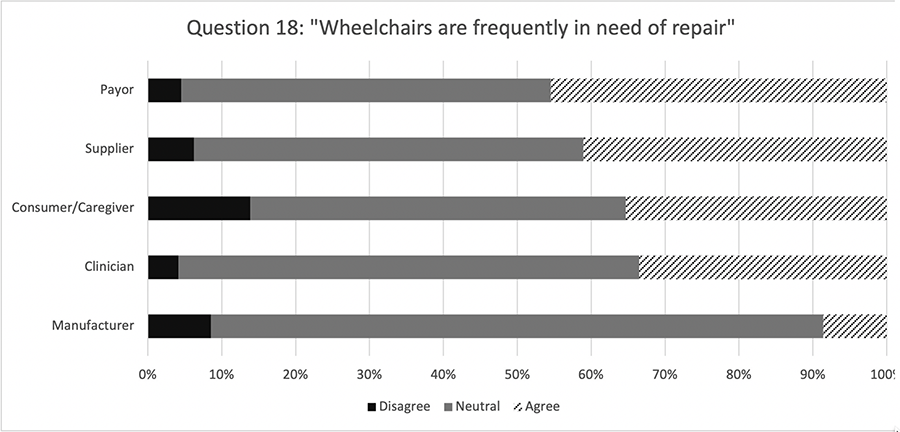
The ability to acquire and maintain high quality, durable CRT devices are crucial to participation in daily life for people with disabilities. The results from this study, which we believe is the first of its kind when considering the breadth of stakeholders, show that there are many flaws in the repair and maintenance process, and it does not work well for any stakeholder group. It is interesting that payors have the highest number of negative responses, since it is assumed that they have the most control in terms of service delivery policy and funding. Other than physician authorization, repairs are usually delayed due to funding reasons such as slow insurance authorization and lack of reimbursement for suppliers providing the repair service.[6] The issue of the lack of reimbursement provided for suppliers repairing wheelchairs can be seen in the results of Question 18 (Figure 3), where they were the group with the second highest number of negative responses. The article by Schmeler & Dicianno (2022) mentioned the large amount of unbillable time that occurs for repair technicians, and how most suppliers provide repair services at a financial loss and do it solely for customer retention.[3] When considering questions that involve the process of repair and maintenance (Figures 1 & 2) and not the durability of wheelchairs, it is worth noting that suppliers' and manufacturers' responses seem quite neutral, even though they are the stakeholders that are directly involved in repair and maintenance of devices other than the consumers themselves who use the devices. It was expected that the group with the highest number of negative responses would have the lowest number of positive responses, and vice versa, but this is not the case in any of the questions analyzed. This could be attributed to the fact that these questions are fairly vague, so respondents could have interpreted them differently, and elaborated more on their responses in the comment box provided in the questionnaire.
CONCLUSION
Based on the findings of this study, the repair and maintenance process in CRT service delivery is incredibly flawed, and the durability of the wheelchairs are not meeting the expectations of the stakeholder groups. Overall, the durability, repair, and maintenance of CRT are not performing to the satisfaction of any stakeholder group and reform is needed to improve the efficiency and feasibility of the CRT service delivery process. The lack of satisfaction with the CRT service process suggests that there are opportunities for emerging and novel CRT service delivery process and policy models that directly impact multiple stakeholders and supports the independence of individuals with mobility impairments.
REFERENCES
[1] Complex Rehab Technology Definition. (2014, June 1). National Coalition for Assistive and Rehab Technology. https://ncart.us/uploads/userfiles/files/CRT%20Definition%206-1-14.pdf
[2] Betz, M., DiGiovine, C. P., Galbreath, P., Stojkov, A., Berner, T., Hibbs, R., & Schein, R. M. (2022). Service delivery for complex rehabilitation technology: A scoping review. Disability and Rehabilitation: Assistive Technology, 17(8), 853–871. https://doi.org/10.1080/17483107.2022.2111609
[3] Schmeler, M. R., & Dicianno, B. E. (2022). Viewpoints on the scoping review for the development of a novel coverage and service delivery policy for complex rehabilitation technology. Disability and Rehabilitation: Assistive Technology, 17(8), 872–874. https://doi.org/10.1080/17483107.2022.2113457
[4] Beauregard, T., Schein, R. M., Berner, T., & DiGiovine, C. P. (2022). Development of an online questionnaire examining stakeholder perception of the CRT service delivery process. 2022 Rehabilitation Engineering and Assistive Technology Society of North America Virtual Conference. 2022 Rehabilitation Engineering and Assistive Technology Society of North America Virtual Conference, Virtual. https://www.resna.org/sites/default/files/conference/2022/SeatingandMobility/StudentScientific/93_Beauregard/93_Beauregard.pdf
[5] RESNA Wheelchair Service Provision Guide. (2011). https://www.rstce.pitt.edu/RSTCE_Resources/RESNA_PP_WSProvisionGuide2011.pdf
[6] Ruffing, J. J., Schmeler, M. R., Schein, R. M., & Mhatre, A. (2022). A cross-sectional descriptive analysis of complex rehabilitation technology (Crt) supplier opinions on the current state of wheelchair repair services. Disability and Rehabilitation: Assistive Technology, 1–6. https://doi.org/10.1080/17483107.2022.2121007
ACKNOWLEDGEMENTS
The contents of this publication were developed under a grant from the National Institute on Disability, Independent Living, and Rehabilitation Research (NIDILRR grant number 90DPGE0014-01-00).
In addition, the authors want to acknowledge the 'R1 Scoping Discovery Review of Complex Rehabilitation Technology (CRT)' project team that also included Rich Schein, Theresa Berner, Madelyn Betz, Rachel Hibbs, Melissa Wright, Ashley Stojkov, and Mark Schmeler for their contributions and support.