Miranda Noack1, Madeline Blankenship1, Amy Zhang1, Cathy Bodine1
1University of Colorado Denver Anschutz
INTRODUCTION
Wheelchair users are estimated at 70 million people worldwide, with more than 3 million users in the US alone [1-3]. While the primary purpose of wheelchairs is to increase mobility, a wheelchair also promotes social inclusion, provides postural support, reduces the progression of deformities, and improves a user's overall quality of life [4-5]. Further, people who use wheelchairs can spend upwards of 16 hours a day in their chair [6], increasing their risk of developing asymmetrical sitting postures that can negatively impact their health and function [4, 7-8]. There is great need for wheelchair design to focus directly on each user, accommodating both their postural and functional needs, as well as overall comfort.
Clinically, pelvic position is one of the most important measures in evaluating seating systems for wheelchairs. Accommodating or correcting a non-neutral pelvic posture is the basis for reducing detrimental postural compensations higher in the body [9]. The international standard, ISO 16840-1:2006, uses angular measurements of body segment orientation to objectively describe a wheelchair user's sitting posture. Additionally, wheelchair seating support surface angles are defined, allowing body segment angles to be correlated to the seating support surfaces of the wheelchair.
Due to the nature of wheelchair fittings, users are typically assessed from within their chair. The current standard of practice utilizes goniometers to measure angles of two related body landmarks, such as the iliac crest, relative to the seat to measure body segment angles. Large amounts of soft tissue and the inability for clinicians to see the landmarks leads to poor interrater reliability of body measurements between clinicians. This suggests that it would be valuable to improve the measurement accuracy of body landmarks and body segment angles. However, more novel alternatives that improve accuracy, such as motion capture and articulating arms [7], fail to transition from research to clinical use due to complexity, cost, or errors that arise in realistic settings outside of a research laboratory.
Therefore, there is a critical need to develop a more accurate, low cost, and easy-to-use device that enables clinicians to assess the seated posture of a user being fitted for a wheelchair. The purpose of this research was to develop a proof-of-concept ultrasonic trilateration system for digitizing anatomical landmarks and calculating body segment angles. Ultrasonic ranging shows great potential as a low-cost measurement system capable of clinical implementation. Paired with the right localization method, the system has the potential to fill a much-needed gap in clinical assessments for seated posture measurement.
DESIGN AND PROTOTYPING

The first step towards a proof-of-concept ultrasonic trilateration system was designing a 3D localization system to be used to digitize anatomical landmarks on a seated patient within a clinical environment. Ultrasonic sensors can send and detect signals through various mediums, including metal, overcoming the line-of-sight challenge of current systems [11]. Additionally, the low cost and recent advances improving accuracies for ultrasonic ranging and localization, have prompted researchers to explore clinical applications of ultrasonic sensing.
For the proof-of-concept design, the HC-SR04 ultrasonic distance sensor was selected due to its wide availability, affordability (<$2-4 each), and working specifications (range 1-400 cm, measuring angle 15 degrees, accuracy 3 mm).
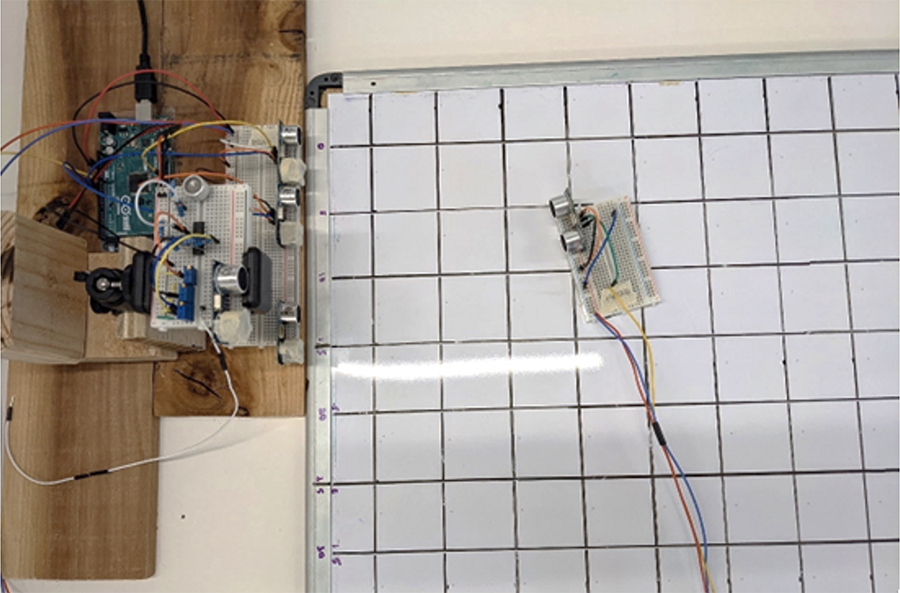
Despite being designed as an all-in-one transmitter and receiver, we implemented off-label, mobile transmitter localization. Rather than a single sensor transmitting and receiving a signal, we manually programmed one sensor to act as a transmitter and four sensors to act as receivers, one at the origin, two offset in the y-direction, and one offset in the z-direction. Having receivers placed in two dimensions mimics a setup in which the receivers are placed on a flat surface such as a clinic ceiling. In all cases, signal processing was done with an Arduino Mega 2650 using time-of-arrival (TOA) measurements to determine the distance, where distance is ½ TOA times the speed of sound (34 cm/s).
The second step towards a proof-of-concept ultrasonic trilateration system was to select a multilateration method to digitize the anatomical landmarks and calculate body segment angles. Multilateration uses the known locations of at least three reference points and the measured distances from each to a target to determine the coordinates of the target. Realistic environments have measurement error which can be addressed by adding additional reference points. We used four receivers as reference points. In order to calculate the best fit "trilateration" with four data points, we used least squares to find the best fit target transmitter coordinates given the four distances measured by the receivers [11]
To determine the viability of the ultrasonic trilateration system we conducted a series of calibration and validation tests. Once each sensor was individually calibrated, they were arranged in the 3D space to capture measurements in each plane (x, y, z). The receivers were arranged in an array in the y- and z-planes of a 3D coordinate space, as if affixed to a clinic wall or ceiling. Distance measurements were computed as the transmitter moved through a 60x90cm grid at 10cm intervals in the x- and y-planes. Measurements that were outside of the reachable area of the sensors were discarded. We used least squares multilateration to calculate the estimated coordinates of the transmitter. Finally, we compared the estimated coordinates of the transmitter to the true coordinates of the transmitter. The mean absolute error of the Euclidean distance between the estimated and true coordinates was used as a metric of measurement accuracy.
RESULTS AND DISCUSSION
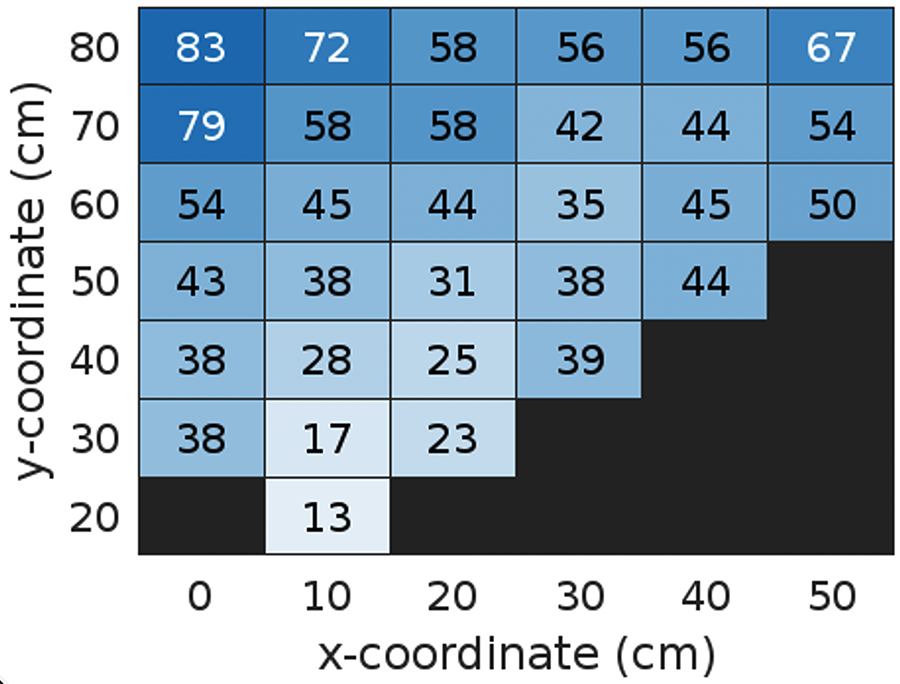
Due to the narrow measuring angle of the HC-SR04 sensors and the placement of the receivers in this initial prototype, there were regions on the testing setup that were undetectable. The sensors measured distances in approximately 65% of the testing area.
The measurement error, calculated as the mean absolute Euclidean distance between the estimated and true transmitter coordinates, ranged from 13cm to 86cm with a mean of 47cm. A measurement accuracy of 13cm is not a significant improvement on today's standard of care using goniometers. Furthermore, the error increased as the target moved away from the receiver array. This suggests that at even further distances, such as those in a clinical environment, the amount of error may continue to increase to amounts that make a device made out of these sensors prohibitively inaccurate.
Although this seems like high variability, Figure 3 also reveals that error is the smallest in the central area with coverage from multiple receivers. Given the inexpensive nature of this type of sensor, it would be interesting for future iterations of this device to compare the performance of a large number of low quality sensors to the performance of a device built with a small number of high quality sensors. Furthermore, error could be minimized by calibrating the angles between the transmitter and receivers.
CONCLUSION
The purpose of this research and development project was to develop an alpha prototype objective measurement tool for assessing seated posture during wheelchair seating and positioning assessments that used ultrasound 3D localization to digitize the anatomical landmarks of a seated patient with the intention to objectively measure relative and absolute body segment angles. Ultrasonic localization has strong potential for being a low-cost anatomical landmark digitizer that can provide objective measures for clinicians performing wheelchair seating and positioning assessments. However, no real world configuration of this particular receiver and transmitter is likely to measure with clinically relevant accuracy. Therefore, we do not recommend the use of the HC-SR04 for the development of a clinical measurement tool for wheelchair seating and positioning assessments.
REFERENCES
[1] World Health Organization and World Bank, "World Report on Disability," Dec. 2011. [Online]. Available: https://www.who.int/publications/i/item/9789241564182
[2] A. M. Karmarkar et al., "Demographic profile of older adults using wheeled mobility devices," J. Aging Res., vol. 2011, Jun. 2011, doi: 10.4061/2011/560358.
[3] S. Erika, "Americans With Disabilities: 2002," US Census Bur., p. 33, May 2006.
[4] A. Davies, L. H. D. Souza, and A. O. Frank, "Changes in the quality of life in severely disabled people following provision of powered indoor/outdoor chairs," Disabil. Rehabil., vol. 25, no. 6, pp. 286–290, Jan. 2003, doi: 10.1080/0963828021000043734.
[5] WHO and USAID, "Guidelines on the Provision of Manual Wheelchairs in Less Resourced Settings," Organización Mundial de la Salud, Ginebra, 2017. Accessed: Oct. 03, 2021. [Online]. Available: https://apps.who.int/iris/handle/10665/274141
[6] A. M. Cook and J. M. Polgar, Assistive Technologies: Principles and Practice, 4th ed. Elsevier Inc., 2014, p. 480.
[7] S. J. Hillman and J. Hollington, "A quantitative measurement method for comparison of seated postures," Med. Eng. Phys., vol. 38, no. 5, pp. 485–489, May 2016, doi: 10.1016/j.medengphy.2016.01.008.
[8] D. Gavin-Dreschnack, L. Schonfeld, A. Nelson, and S. Luther, "Development of a screening tool for safe wheelchair seating," vol. 4, p. 12.
[9] M. Malagodi, D. Hobson, and K. Mostafa, "Task: S-3 Non-invasive Monitoring of Spinal/Pelvic Alignment," University of Pittsburgh, Rehabilitation Engineering Research Center on Wheelchair Mobility. Accessed: Oct. 02, 2021. [Online]. Available: http://rercwm.pitt.edu/RERCWM_Int/RERCWM_Int_RERC1/RERC_Int_RERC1_pdf/finalreport.pdf#page=63
[10] M. Toa and A. Whitehead, "Application Note: Ultrasonic Sensing Basics." Texas Instruments, Sep. 2019. Accessed: May 26, 2022. [Online]. Available: https://www.ti.com/lit/an/slaa907d/slaa907d.pdf?ts=1653524052099
[11] Norrdine, A. (2012, November). An algebraic solution to the multilateration problem. In Proceedings of the 15th international conference on indoor positioning and indoor navigation, Sydney, Australia (Vol. 1315).
ACKNOWLEDGEMENTS
We would like to thank Brecca Gaffney, Kelly Waugh, and Zhengxiong Li for their dedicated advising and mentorship.