TOASTI: Tongue-Operated Assistive Instrument
Justin Wangying Lam, Sophia Shan, John McNamee, Arnav Bhat, Mohamed Mohamed
Problem Statement / Research Questions and Background
Individuals with paralysis need to be able to conduct activities of daily living (ADLs) and contact help if an adverse event occurs. These patients may need certain devices to help them with ADLs, such as getting dressed, using the restroom, and eating meals. For instance, specialized wheelchairs with head controls could allow quadriplegics to move independently. However, the current market does not have a life-alert and communication device for patients who have paralysis. People with quadriplegia or paraplegia could benefit from a device that allows them to communicate with others and call for help in emergency situations.
Individuals with limited control of their limbs usually have difficulties with tasks that require fine dexterity. However, many assistive devices require fine motor skills. The scope of our target population is not insignificant: about 5.4 million people in the United States were living with paralysis (Armour, 2016). About 250,000 to 500,000 people suffer from a spinal cord injury every year, with older adults of ages 70 and above being the highest at-risk group (World Health Organization, 2013). In particular, quadriplegia occurs in 60% of traumatic spinal cord injury cases (Cleveland Clinic, 2021). Some patients with quadriplegia may also lose functioning of muscles involved in respiration and vocal cord movements (Mohapatra and Rout, 2019).
Prior to the development of our device, we examined the market for any existing technologies that help patients contact emergency services. An example medical life system is the Medical Guardian system. The device is a wearable pendant, which has a button and speaker system that reaches the company's call center. The cost is around $149.95 with a monthly fee of $39.95 (Schlenker and Hoyt, 2022). Another example of a life alert is MD Sense, a system of sensors in the home environment. When a user falls, the sensors send signals to a monitoring center. Users who are unable to use their hands due to their position, such as front-facing falls, can still get the help they need. The device is a hands-free solution to get help, but patients cannot use this device outside their home or in public spaces (Essence Smartcare, n.d.).
We also looked at current types of alternative communication devices for people with paralysis. These broadly include switch-based control devices, mouse emulation, and automatic speech recognition (ASR). A switch-based control device often uses a binary "Yes" / "No" categorization, but some researchers have also used Morse code to obtain a wider range of feedback. A mouse emulation device provides a hands-free alternative to interfacing with computers, but the muscles used for the device, such as facial muscles, can be awkward and clumsy to reach the desired output. Automatic speech recognition also has several contraindications, such as its difficulty to use such systems in adverse environments (Pinheiro, Naves, Pino, Andrade, & Bourhis, 2011).
Our research project aimed to address the unmet communication needs of patients with paralysis. A hypothetical device should (1) be able to send out life alert messages and (2) interface with computer devices to facilitate communication with other people.
Methods/Approach/Solutions Considered
Compared to other systems we have examined, our proposed device uses bioelectrical signals, specifically those from an analog electromyogram (EMG) sensor. It mostly closely resembles previous switch-based control devices, but it consists of both life alert and communication capabilities. It also does not require the use of a conductive gel to enhance conductivity, which allows for its quick application to different body parts.
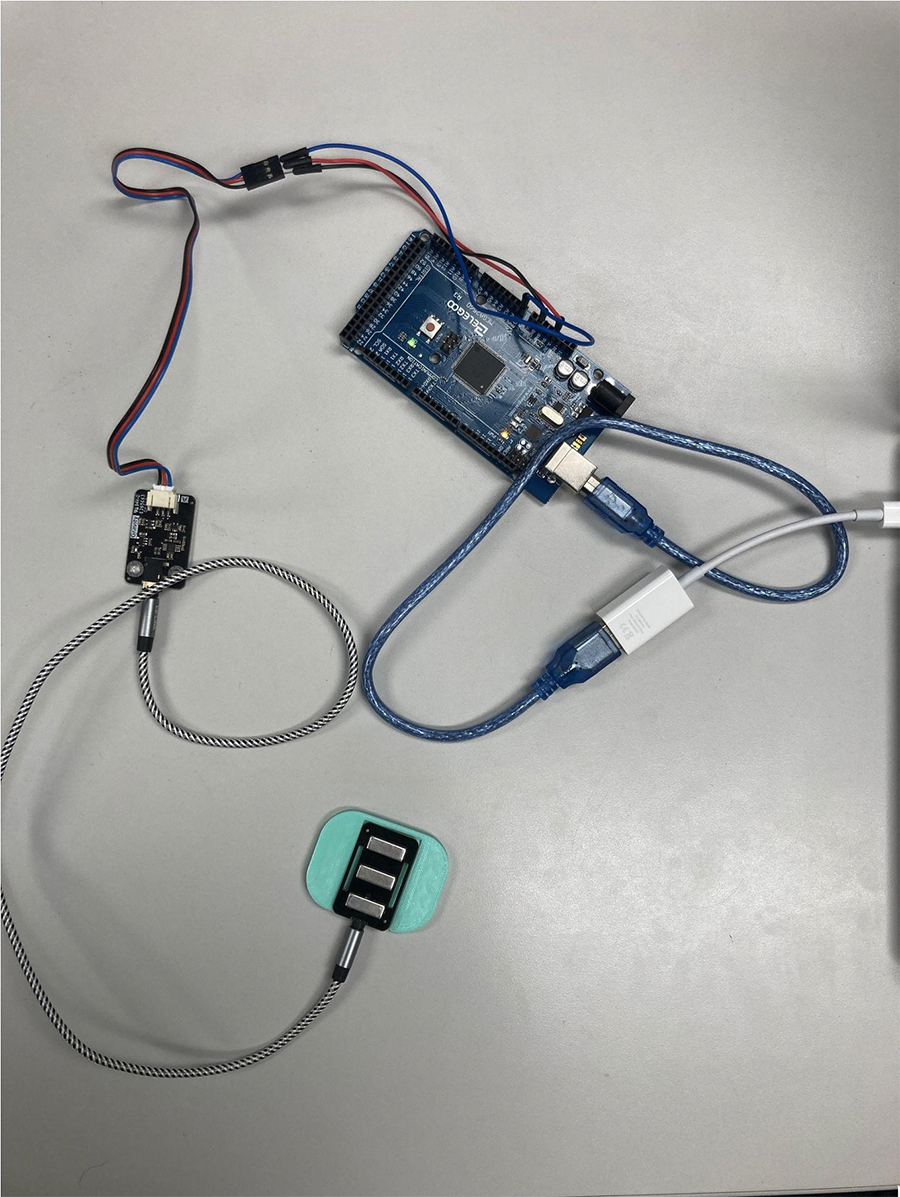
The first iteration of our product used machine learning methods to process raw signals from the analog EMG devices. When the raw EMG signals were collected, they needed to be preprocessed in MATLAB: the data was squared, normalized, smoothed using an in-built MATLAB function called "loess", and finally amplified by a factor of 10. The data was processed through a threshold detection algorithm, and the activation requirement for an alert was three signals, which correspond to three consecutive tongue movements. The interface of our product was an Arduino board, and the focus of our project was the experimentation of different casings for the EMG sensor to ensure secure attachment (Figure 2),
While the first iteration showed that the concept could work, it required the signals to be recorded prior to its analysis in MATLAB. The next iteration of our product aimed to use the functional capabilities of the microcontroller in capturing live-stream data. This involved improvements in our firmware to interpet live-stream data, and this can send alert signals in real time. We also developed the "Yes" or "No" functionality of our device. In this case, the machine learning methods were not used, and instead, baseline data of electromyogram signals was taken from the participant over the time period of three seconds.
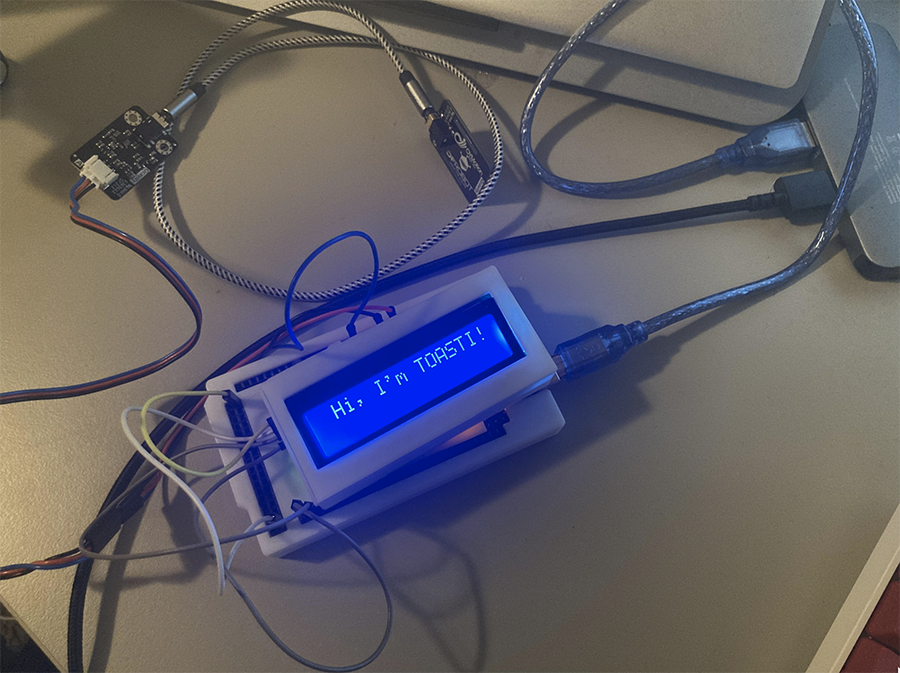
Later iterations of our product saw the improvement of our product's physical design, which included a proper casing for the electrical components of our device. It also involved the addition of a liquid crystal display (Image 2).
Future iterations of our product will involve the translation of MATLAB code to Python, as Python is a free, open-source language that could have the same functionality as MATLAB. This will help enhance the accessibility of our software, and it would lower the financial barriers to the device. We also plan on developing code for the liquid crystal display that will demonstrate
Description of Final Approach and Design
The tongue-controlled life alert system will use an analog electromyogram (EMG) sensor to track muscle movements. Our project title name is an artifact of previous iterations of our product. While we initially thought of capturing the muscle signals of the tongue pressing against the cheek, the sensor can realistically be applied to any location on the outside skin of the user's body, as long as the user has control over the muscles in that region. Current recommendations for regions of contact include the masseter muscles (clenching and releasing the jaw), the carotid muscle (moving tongue in one direction), and the wrist muscles (clenching and releasing a closed fist). The EMG sensor collects electrical activity in the region of contact, and these signals can be identified in this area.
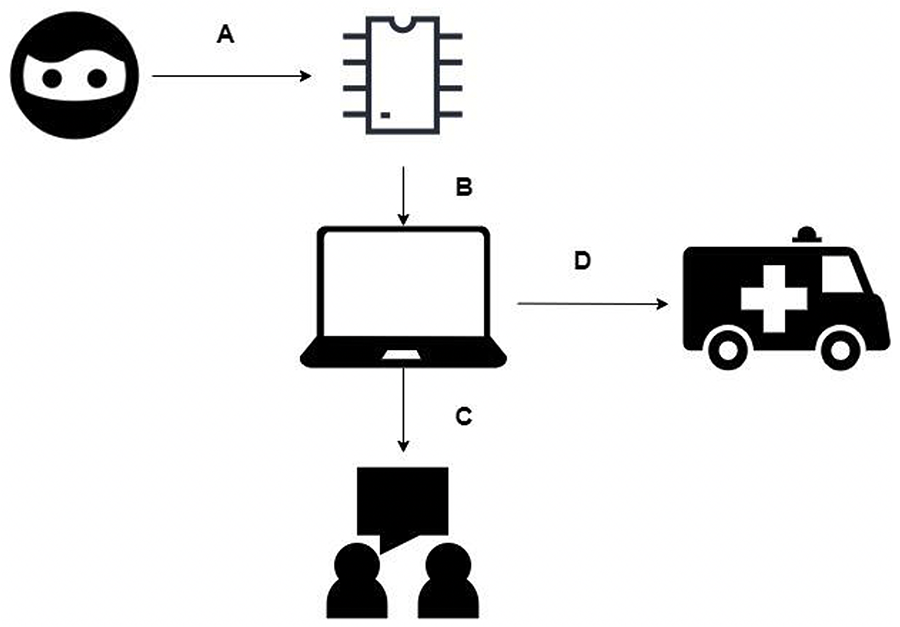
As the sensor collects the data, a MATLAB program analyzes that data to determine specific set patterns by identifying specific inflections in the dataset. Throughout this process, EMG signal data is live-streamed onto the computer, and it is visible for users to see. A three-second initialization period is used as the basis for a "resting" state. Then, the specific "pattern" is considered to be one contraction for "No" and three contractions for "Yes". These cues appear as a display on the computer screen. Finally, if the program identifies the set emergency pattern, it will automatically initialize contact to a trusted friend or family member, similar to current life alert systems (Figure 1).
Outcome Testing
The device, as pictured in Figure 2, showed promising results in the early stages of our development. We were able to accurately obtain EMG signals from the three locations that we tested (cheek, neck, and wrist), and the software was able to communicate with the device to produced the desired output (i.e. "Yes" / "No" signals and contacting emergency services).
Nine participants were recruited for individual outcome testing of our device. A group of peer mental health advocates (n = 6), disability advocates (n = 2), and a M.S. in Orthotics and Prostheses candidate were surveyed for use of this device. Thematic analysis was performed to identify key problematic areas for TOASTI.
One challenge that our test users faced included receiving proper signals. Some (n = 5) were able to receive signals using either the masseter or the carotid muscles, while the rest had to use their wrist muscles. One user suggested different avenues of input, such as the use of "machine learning algorithms to detect emotions on a user's face". Another concern of test users was the feasibility of EMG sensor attachment. A user expressed concern over the feasibility of having long-term contact with an electrode, and they suggested that they would be worried about type 1 pressure injuries or pressure ulcers. Another user found it "really difficult to make sure the device stays on".
Despite their concerns, all users agreed that the device showed promise in the ability to serve as an alternative communication device for patients with certain communication disorders, mobility disabilities, and other health conditions. One of our test users thought that the broad applicability of the EMG sensor was a "huge plus". Another user complimented the software, saying it was "a great idea to have this kind of user interface… it makes it so clear on what is going on."
Future iterations of our product would take into the usability concerns of our test population. Ideally, the electronics would be covered in a waterproofed container. User satisfaction may also be enhanced through the use of different fastening mechanisms, depending on the areas of target.
Cost
The cost of materials in assembling the device can be found in Table 1. Some parts have not been fully assembled, such as the display and the 3D printed case, but these are intended to be parts of the final project.
| Item | Cost |
| Elegoo MEGA 2560 Board | $21.00 |
| DFRobot Gravity: Analog EMG Sensor | $49.50 |
| LCD 1602 Display | $5.59 |
| 3D Printed Case | $16.00 |
| Total | $92.09 |
The next steps to reduce the cost of the device would be the development and production of a PCB and an analog EMG sensor, which could minimize the cost of procuring a microcontroller board. The expected price of the device would be a one-time expense of $100, with the difference used for any modifications to the casing of the device. If users are interested in assembling this device on their own, the software and listings of parts that we have used will all be publicly available on our website.
We have also looked into possible payment methods through insurance for this device. As one of our target populations could be older adults, Medicaid could off-set some of the device prices. Depending on the state, home and community based services (HCBS) may offer coverage. Consumer directed services offer an allowance for Medicaid patients, which could be used for paying a life alert device. Most states also have a "Money Follows the Person" program, which operates similarly to the HCBS program, but it is designed for older adults. Unfortunately, Medicare programs that patients are enrolled in are not likely to cover medical life alert devices because they primarily cover in-patient care (Schlenker and Hoyt, 2022).
Private insurance generally does not cover medical alert systems, but it can vary based on the company's policies. Advocacy organizations, such as the AARP or Area Agency on Aging, may also assist in helping older patients obtain the life alert system they need. The state's Department of Mental Health may also help connect residents with the support they need for personal self-care (Caring, 2022). If the patient qualifies, Veteran Affairs can also help purchase a medical life alert (Senior Safety Reviews, 2021).
Significance
There is a global need for current life alert systems: the market for medical alert systems was valued at nearly $6.5 billion USD, and is expected to triple to nearly $21 billion USD by 2030 (Avinash et al., 2021). The need for such devices may also grow, as the number of patients with paralysis increase. Nearly 1 in 50 individuals live with some form of paralysis, and over 10,000 individuals suffer quadriplegia-causing injuries every year in the United States alone (Christopher & Dana Reeve Foundation, n.d.). Over 17,000 individuals are affected by some spinal-cord affecting injury, which leads to paraplegia in the best-case scenario (Sci-Info-Pages, 2019).
However, current life alert systems only allow some users to access emergency services when needed. Passive monitoring systems, such as sensors that indicate falls or detect heartbeat, may be unreliable and are not comprehensive in covering all life alert emergencies. Active monitoring systems, such as those that are activated by the use of a button, may not be easily activated or accessible to those with quadriplegia.
TOASTI will enable those with paralysis or communication disorders to live more independently, especially in community-based settings where patients may not always have around-the-clock in-person monitoring. The system we designed is also a marked improvement over other medical life alert devices. Since our device is designed to be able to read three signals from muscle contractions on most parts of the body, a large user population can access this life-saving technology. With the manufacturing cost of this device being low, the device can be reasonably priced for commercial sale, making the device widely accessible to those with paralysis.
References
Armour, B. S., Courtney-Long, E. A., Fox, M. H., Fredine, H., & Cahill, A. (2016). Prevalence and Causes of Paralysis—United States, 2013. American Journal of Public Health, 106(10), 1855–1857.https://doi.org/10.2105/AJPH.2016.303270
Avinash, S., Himanshu, J., & Vineet, K. (2021, December). Medical Alert Systems Market Size, Share & Analysis, 2021-2030. Allied Market Research.https://www.alliedmarketresearch.com/medical-alert-systems-market-A14983
Caring. (2022). Are Medical Alert Systems Covered by Insurance in 2022? Caring.Com.https://www.caring.com/best-medical-alert-systems/are-medical-alert-systems-covered-by-insurance/
Christopher & Dana Reeve Foundation. (n.d.). Paralysis statistics. Reeve Foundation. Retrieved December 5, 2022, fromhttps://www.christopherreeve.org/living-with-paralysis/stats-about-paralysis
Cleveland Clinic. (2021, June 10). Paralysis: What Is It, Diagnosis, Management & Prevention. Cleveland Clinic.https://my.clevelandclinic.org/health/diseases/15345-paralysis
Essence Smartcare. (n.d.). A new dimension in fall detection. A Better Way To Detect Seniors Falls. Essence SmartCare. Retrieved December 5, 2022, fromhttps://www.essencesmartcare.com/products/mdsense-fall-detector/
Live Life Alarms. (2019, April 11). 4G Mobile Personal Medical Alarm Pendant | Live Life Alarms.https://livelifealarms.com.au/product/order-4gx-mobile-alarm/
Mohapatra, B., & Rout, N. (2019). Dysarthria Consequent to Cervical Spinal Cord Injury and Recurrent Laryngeal Nerve Damage: A Case Report. Journal of Rehabilitation Medicine - Clinical Communications, 2, 1000022.https://doi.org/10.2340/20030711-1000022
Pinheiro, C. G., Naves, E. L., Pino, P., Losson, E., Andrade, A. O., & Bourhis, G. (2011). Alternative communication systems for people with severe motor disabilities: A survey. BioMedical Engineering OnLine, 10, 31. https://doi.org/10.1186/1475-925X-10-31
Schlenker, L., & Hoyt, J. (2022, November 15). Medical Guardian Cost & Pricing in 2022. SeniorLiving.Org.https://www.seniorliving.org/medical-alert-systems/medical-guardian/
Sci-Info-Pages. (2019, June 12). Spinal Cord Injury Facts & Statistics. Spinal Cord Injury Information Pages.https://www.sci-info-pages.com/spinal-cord-injury-facts-and-statistics/
Senior Safety Reviews. (2021, March 9). Are Medical Alert Systems Covered By Insurance? SeniorSafetyReviews.Com.https://www.seniorsafetyreviews.com/are-medical-alert-systems-covered-by-insurance/
World Health Organization. (2013, November 19). Spinal cord injury.https://www.who.int/news-room/fact-sheets/detail/spinal-cord-injury